
By Timmy Broderick
Data visualizations by Kevin Huber
“March 22, 2017. Right then, everything changed.”
Shelley’s raspy voice falters, her eyes misty.
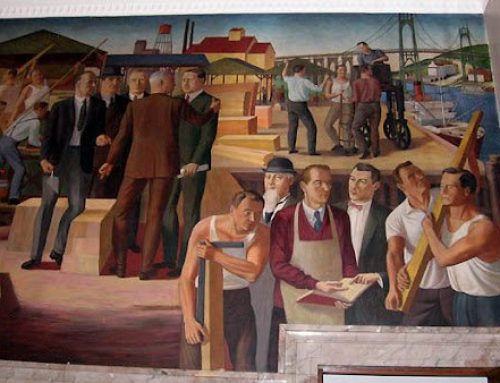
We are sitting in a red booth inside a McDonald’s in Delhi Township, a suburb on the west side of Cincinnati. Across from us — carving figures into his styrofoam cup — is her 13-year-old son, Chance. He remains quiet as his mother details how, in less than 24 hours, she overdosed, watched her best friend die, and lost custody of her son.
(To protect their privacy, Shelley requests that I only use first names.)
The tragedy, according to Shelley, started soon after Chance left for school. Her and her best friend, Ryan, decided to snort heroin, but they quickly OD’d. Their dealer had actually sold them carfentanil, a synthetic opioid 5,000 times stronger than heroin.
Shelley was lucky; paramedics revived her. Ryan — a man Chance still calls uncle — was not so fortunate.
“I remember coming back to the house that day and I found all the remnants,” she says. “Not only was he gone, but I’m sitting there picking up the ambulatory scissors, the heart sticky things. It was another smack in the face, like,‘Wow, this isn’t a dream.’”
“We’re calling people 24 hours a day,” says Moira Weir, whose job it is to find homes for this surging population of minors impacted by the opioid crisis. “We have kids sleeping in the office.”
As his mom recounts these events, Chance promptly gets up to refill a mostly-full drink. Later, I ask him for his version of that day.
He pauses, looks out the window, then turns toward his mother.
“I was there,” he says. “I seen you fall out in front of me, then I went to school.”
Shelley hadn’t known. She starts to apologize, but that only upsets Chance.
“Dang, I didn’t know you could forget this,” he says.
“How was I supposed to know? I was out of it,” says Shelley.
The bickering continues for several minutes until both run out of steam. The silence reinforces the cruel irony of a shared trauma perfecting one memory while dulling the other.
Chance’s grandparents picked him up from school that day. He spent three months with them but then was placed in foster care, where he now spends most nights while his mother endeavors to prove to the state that she can stay sober and be a fit parent.
***
Shelley and Chance’s story is not uncommon in Ohio, a state that is second in the nation only to West Virginia in opioid overdose rates. In Hamilton County in Southwest Ohio, the problem is acute, especially when looking at the impact on children. In 2006, there were 1,920 Hamilton County children in state custody, according to Hamilton County Jobs and Family Services (HCJFS). Over the next eight years, that number only grew by some 200 children. Between 2014 and 2016, the number ballooned to a 20-year high of 2,918 kids in state custody. Nearly 700 have entered the system since then.

Above: 13-year-old Chance, whose mother’s opioid abuse landed him in foster care; Top photo: Chance and his mother, Shelley. [Photos by Timmy Broderick]
A lack of safe homes is a serious problem for these “opioid orphans” — some literally orphaned, others displaced from parents in the throes of addiction or caught up in the criminal justice system — but perhaps more troubling is the trauma these kids have endured.
“We’ve had children who have helped their parents shoot up, we have had children who have lived with parents who have been deceased for two days, not knowing that because they’re so used to their parents being passed out,” says Weir.
Trauma is not just terrible to live through; it also offers a grim prognosis.
According to a landmark study published in 1998, children with four or more adverse childhood experiences (ACEs) face double the risk of stroke and heart disease, are 10 times more likely to inject drugs, and are 12 times more likely to attempt suicide.
(Take this questionnaire and find out your ACE score.)
Trauma is not just terrible to live through; it also offers a grim prognosis. With an exorbinate number of minors being impacted by the opioid epidemic in Hamilton County, the region could wake up in 15 years to another public health crisis.
“It matters how many bad things happen to you,” says Dr. Mary Greiner, a pediatrician at Cincinnati Children’s Hospital (CCH) who specializes in child abuse and childhood trauma. “If lots and lots of bad things are happening to you as a child, it’s going to affect your entire life.”
With an exorbitant number of minors being impacted by the opioid epidemic in Hamilton County, the region could wake up in 15 years to another public health crisis.
***
In Southwest Ohio, the opioid epidemic is not just impacting children like Chance; it’s also impacting children before they are born, like Lincoln Carr.
For the first seven and a half months of her pregnancy, Lincoln’s biological mother was a daily heroin user. She only found out about the impending childbirth because she was arrested for drug possession and paraphernalia. She was put on methadone to help treat her addiction. When Lincoln was born a month later and the umbilical cord was cut, his body went into withdrawal.
“You watched him and he would just screech in pain,” says Stevi Carr, his adopted mother. “I remember there was this one time where his whole body was shaking. They would bring in warm blankets and try to swaddle him to keep him compact, keep pressure on him to try and simulate the womb.”
Lincoln was suffering from neonatal abstinence syndrome, or NAS, an umbrella term that denotes any infant exposed to drugs in-utero and, after birth, exhibits withdrawal symptoms.
While it is not a new diagnosis, it is gaining newfound attention because of the opioid epidemic. National rates have soared 400 percent since 2000. In Greater Cincinnati, the number of infants born dependent on drugs increased by 227 percent from 2012 to 2014.
Lincoln’s biological mother was a daily heroin user. When Lincoln was born and the umbilical cord was cut, his body went into withdrawal.
Dr. Stephanie Merhar, a neonatologist at both CCH and St. Elizabeth’s Hospital in Northern Kentucky, says that sometimes half of the babies she sees in NICU will be suffering from NAS.
Typical symptoms include insomnia and inconsolable crying, while more severe cases include tremors. If the infant checks enough boxes, they will be diagnosed with NAS, though what determines the severity of the symptoms remains unknown.

Lincoln Carr, who was born addicted to opioids. [Photo by Timmy Broderick]
Neonatal intensive care units are, almost uniformly, not pleasant. Crying babies wail for their mothers and loud machines whirr without end — hardly a conducive environment for a newborn in withdrawal.
Multiple studies have shown that keeping mom and baby in the same room, what is called “rooming-in,” dramatically decreases NAS symptoms and shortens recuperation time.
“If there’s one room, one mom, with her baby and she can breastfeed and hold her baby every time he or she cries, that makes sense that those kids are going to need less treatment,” says Merhar.
Proven solutions are not always easy to implement, however.
“Ironically, it’s one of the populations of moms least able and least likely to do that,” says Merhar.
Private, inpatient medical centers like Brigid’s Path in Dayton, Ohio, have opened to address the problem. They combine drug treatment with separate, quiet rooms and swaddling to sooth the babies’ pain.
Unfortunately, pharmacological treatments lack a similar consensus, although many NAS-afflicted infants do receive a kind of opiate to ease the pain of withdrawal.
When it comes to the long-term effects of NAS on children, Merhar says there’s a dearth of studies on the subject. “Nobody really knows,” she says.
A group of Australian researchers have demonstrated an association between NAS and lower academic performance, but they did not investigate biological causes.
To that end, Merhar is seeking funding for a study to track the effects of opioids on infant brain development from six weeks to two years old. Right now, she says, the sprawling nature of the crisis is dizzying, making it hard to know what to tackle first.
“Should we be focused on a different medicine to treat mom with, should we be focused on treatment postnatally, keeping the kids with their families, parenting skills — nobody really knows where to focus resources,” she says.
That uncertainty could change as the Ohio Perinatal Quality Collaborative, a group of pediatric physicians across the state, works to standardize care and share best practices.
According to Dr. Michael Marcotte, a neonatologist at Good Samaritan Hospital in Cincinnati, one of the complications to treatment is the rise of fentanyl, an opiate 50 times more powerful than heroin. During the first two months of 2017, 90 percent of unintentional overdose deaths in 25 Ohio counties involved some cocktail of fentanyl, fentanyl analogs, or both.
“Our patients are not responding the way they used to and I don’t think it’s because we’ve changed anything,” he says. “I think it’s because the drug mixture has really made it much more difficult for patients to stop using because they have so many symptoms of withdrawal.”
One of the complications to treatment is the rise of fentanyl, an opiate 50 times more powerful than heroin. “Our patients are not responding the way they used to and I don’t think it’s because we’ve changed anything.”
Marcotte runs a program called Helping Opiate-addicted Pregnant women Evolve (HOPE). It’s a space for pregnant women to get sober, find counseling, and receive regular prenatal care to ensure a healthier birth and child.
“There’s very few women that we work with that don’t identify as wanting to be a good parent,” he says. “We need the parents, we need the families to be healthy because we don’t have enough resources to care for all these kids in the public sector.”
Healthy living extends beyond physical well-being; it means not having to stress about finding your next meal or a place to sleep.
“I had a patient who delivered her baby after coming back from jail for a felony and she said, ‘You know, I’m working hard to be clean in all this, but where am I gonna live, who’s gonna rent an apartment to me, who’s gonna give me a job?’” says Wedig, who works closely with Marcotte.
To that end, HOPE has partnered with First Step Home, a nonprofit for women suffering from addiction, to create Terry’s Home. The program provides expecting mothers with wraparound services like transportation, housing, and on-site nursing care that continues through the first month of their baby’s life.
Rachel Lyon, Director of Development at First Step Home, says it can be overwhelming to tackle everything at once, but that is, ultimately, what is needed.
“It’s not just addiction; there’s trauma, there’s physical things like housing and food and shelter, there’s need for education,” she says. “There’s a lot to helping people get well.”
Working with moms before they deliver is also key to the baby’s health.
“If we wait until the baby is born, it’s almost too late,” says Marcotte. “If the woman is not in treatment, if she’s not getting effective care, their child is destined for a really difficult life.”

Lincoln with his adopted parents. [Photo by Timmy Broderick]
Stevi Carr tells me that she and her husband originally told their caseworker they didn’t want a child born addicted to opiates. But they were encouraged to give it more thought and consideration, and are happy they did.
“People who can help are typically the most afraid of what they don’t know. And that was me,” says Stevi. “I’m so grateful that I just did some more research and took a chance on it.”
Now, says Stevi, she and her husband are thinking about becoming a foster home for other kids like Lincoln.
These kids aren’t “broken,” she says. “They just need some more love.”
***
If Stevi Carr wants to turn her house into a foster home, she picked an opportune time. Opioids are driving kids like Chance into state custody in record numbers.
The statewide numbers hovered around 12,000 kids for several years until 2013, when more kids started to trickle into the system. Population has since exploded. Public Children’s Service Association of Ohio, a nonprofit advocacy group, says that current state totals fluctuate around 16,000 kids, and the group projects that by 2020 more than 20,000 kids will be in state custody.
Before 2013, the number of kids in Ohio state custody hovered around 12,000. Today, that number is roughly 16,000, with projections of more than 20,000 kids in state custody by 2020.
Kids are staying longer, too. Eight years ago, the average length of stay was 202 days. Today, it is 240 and rising.
Not only are more kids entering the system and staying longer, their trauma is more acute.
“Kids have a more extensive trauma history because of how strong the drug is and how significant the withdrawal symptoms are,” says Michelle Cox, the director of GLAD House in Cincinnati, a nonprofit that provides after-school care for kids in drug-affected households.
According to Angela Sausser, the director of Public Children’s Service Association of Ohio (PCSAO), higher trauma levels force kids into higher levels of care, like residential treatment programs, before they can be placed with a family. This, in turn, winds up costing taxpayers more money.
In 2016, Ohio spent $330 million on foster care placements, half of which went to drug-related cases. If current trends continue, PCSAO estimates that total costs will balloon to $550 million by 2020.
Local agencies will likely be stuck carrying that extra burden. Ohio is the worst state in the country at funding children’s services. In 2014, between federal, state and local funds, the state spent nearly $1.3 billion. Only seven percent came via the state. No other state relies so disproportionately on federal and local dollars — the closest is North Carolina, whose portion accounts for 16 percent.
Ohio is the worst state in the country at funding children’s services.
“It’s frightening,” says Sausser. “We’re really at a crisis here in Ohio when it comes to children’s services not having enough resources to be able to properly care for all the children that are in care.”
Establishing proper care is difficult when service providers themselves are a cause of trauma, says Dr. Mary Greiner, who runs a checkup clinic for kids in foster care.
“The very idea of foster care — to have a stranger come into that environment and take that child away from the caregivers they love, away from that neighborhood, away from that school is extremely traumatic,” she says.
Foster care kids are, by definition, traumatized, to say nothing of what put them in the system in the first place. Greiner treats all of them as if they are at the highest risk because most of them are.
Chance is.
At age six, Chance was hit by a car while riding his bike and suffered a traumatic brain injury. At age seven, his dad and Shelley’s fiancé overdosed on pain medication and died. At age eight, his mother lost her home. At age 11, his mother started using heroin. At age 12, his mother overdosed and his “uncle” died.
Chance has endured a lot, which is why Shelley cuts him slack for his newfound delinquency: skipping school, smoking weed, and slugging a police officer.
According to Greiner, these behaviors, classically seen as “acting out,” are really signs of something else.
“A lot of those behaviors are the way that child is trying to communicate that they have experienced loss and that they are scared and that they feel uncertain about what is happening to them,” she says.
Shelley jokingly calls Chance a “raging storm,” but she is legitimately worried.
“I’m afraid he’s going to be a statistic — not a good statistic, either,” she says.
It’s a valid concern. A study published in 2008 showed that kids on the margin of placement — cases in which child services is unsure whether to remove the child from the home — who entered foster care are two to three times more likely to be arrested, convicted, or imprisoned than those who stayed with their family. And despite the trauma that Shelley has inflicted on her son, their bond is plain to see.
“He’s been gone from me for so long, he’s already got hair underneath his armpits,” says Shelley, talking about missing Chance. “I mean little shit like that, it’s the little things.”
Chance smirks at her, “Hey, you cussin’ in front of me?”
“Yeah right, you throw out f-bombs like Jack Sparrow,” says Shelley.
They start to joke, trading barbs back and forth while laughing.
Shelley starts to describe all the progress she’s making — new job, new car, new house — but suddenly Chance is obstinate, interrupting her at every turn.
Two minutes later, Shelley turns to me and says, “He’s on the verge of coming back and I’m not sure if he wants to.”
“I want to, I want to, I just want to go home now,” Chance says, slamming his deformed styrofoam cup onto the McDonald’s table.
His mother relents, and Chance quickly ducks out of the booth and walks outside without saying goodbye.
Chance is not lying. He wants to be back with his mom. While in foster care, he has a frequent routine: wait until night, jump from the second-story window of his foster home, and then use Kentucky Fried Chicken stores along the four-mile trek to guide his steps.
Foster care kids are, by definition, traumatized, to say nothing of what put them in the system in the first place.
Shelley does not remember the specifics of most of his excursions, but she does remember a night when an out-of-breath Chance showed up at her door and asked her without preamble, “Mom, do you still think about Ryan?”
After Shelley said yes, Chance replied, “Yeah, I do too, but I don’t as much anymore.”
“So that’s showing me at least that maybe the healing and closure has come to him,” says Shelley.
Moments like that give Shelley hope, buoy her spirits, reminding her why she needs to stay sober.
“My faith has been tested,” she says. “I turned my back for a minute.”
Chance knocks on the window from outside, then rubs his hands together for warmth.
Shelley chuckles.
“Alright, Chance,” she says, and she lumbers out into the cold.
***
Three days after I meet Shelley and Chance in McDonald’s, Chance is arrested.
According to Shelley, he refused to return to his foster home, which he hates — it’s unfamiliar and his friends live miles away. He had been with Shelley (he currently splits time between the two), but flipped out when the time came to switch. Chance started throwing rocks at his mom’s window until a neighbor called the police, who showed up and promptly took Chance to juvenile detention.
Shelley sighs.

Chance and Shelley. [Photo by Timmy Broderick]
If she wants Chance to thrive, she may not have a choice. The consensus that kids do better with family is something I heard often in reporting this story.
“Family is built on permanency, it’s built on we’re always together, forever, and we can love and support each other long-term and we know we’re going to be there,” says Greiner. “And that’s not what foster care is.”
Forty-two percent of kids that entered HCJFS care last year lived with kin (family or a close relative) at least part of the year. Relying on kinship care is difficult, however, because families receive no financial support for taking in their niece or grandchild.
“What I would love to see happen at a federal and state level is to have more financial supports to kinship providers,” says HCJFS Director Moira Weir.
“I don’t think I’m ready for him. I mean, yeah, I’m healed and all that, but I’m not ready for him, not ready for the changes.”
Finding a viable relative is tricky with this epidemic.
“We had a case where the grandma had custody and she ended up OD-ing with the child in the bathtub,” she says. “It’s trying to find a family member that isn’t using if we can’t place them with mom and dad.”
For Shelley and Chance, the hope is that Shelley can stay sober long enough to prove to the state that she can be and remain a fit parent. That is why Shelley signed up for “drug court,” a voluntary program set up by the Hamilton County Juvenile Court and designed to help people struggling with drug abuse (called clients) stabilize and reunite with their kids. To graduate, clients must work with caseworkers and lawyers to prove that they are moving towards stability.
But it’s not just about proving yourself to the court. For people like Shelley, a recovering heroin addict, who must recreate a family they, themselves, destroyed, the task is herculean. How do you win back the trust of a son who rightfully blames you for their problems? How do you erase years of trauma that scream at him not to trust you?
Not easily.
According to Dr. Erica Messer, a pediatric psychologist at CCH, the most important thing Shelley can do for her son is to simply be his mom — to listen to him and care for him when he falls.
“We can’t just fix it, but to acknowledge that it happened is important, to acknowledge that it was hard, and still is hard,” says Messer.
I ask Shelley if the stress makes her want to use again.
“No, I don’t feel like using, I feel like, how do I solve this problem,” she says.
She then expands on the thought, saying, “You know, if you take Chance and times it by thousands of children across the Tri-State, it’s utter chaos.”
Timmy Broderick is a journalist based in Cincinnati, Ohio. Learn more about his work at timmybroderick.com.
Kevin A. Huber is an interactive news developer based in Nashville, Tennessee, originally from Cincinnati, Ohio. You can find more of his work and contact information here.
To support more articles like this one, produced by journalists living and working in the region, become a member of Belt Magazine starting at just $5 a month.


I would hope more tax dollars would go toward healing these kids than their parents. beside just feeding, clothing, and sheltering these kids my hope is that they get some counseling (ongoing) to make sure they know it’s not their fault and that their parents made really bad life choices but they don’t have to do the same.